Frequently Asked Questions
By Pam Stephan | Reviewed by Doru Paul, MD
Updated September 27, 2018
Verywellhealth.com
If you are undergoing a mastectomy, you will probably have surgical drains placed. A surgical drain is a plastic or rubber tube that comes out of your incision site. The tube is attached to a hollow rubber ball that collects draining fluid from the healing area.
While you can expect to stay in the hospital for a night or two after your mastectomy, prior to leaving the hospital, your surgery team will give you instructions on how to care for your surgical site properly to prevent infection, as well as explain how to manage your drains until they are removed during a follow-up visit with your breast surgeon.
Let's explore the basics of surgical drains after a mastectomy, including what they look like, how they stay in place, and what their purpose is.
Surgical Drains During a Mastectomy
When you have a mastectomy, your surgeon may place drains in order to prevent the buildup of fluid and help speed up your healing.
Prevention of a Seroma
This is because without drains, fluid may collect in the space where your breast or lymph nodes had been, and this can cause symptoms like pressure and pain. More seriously, when fluid collects without being drained, it may cause a seroma to develop. A seroma is a collection of clear fluid (called serous fluid) within the wound. Seromas can delay wound healing and result in infection and a poor cosmetic outcome.
What a Surgical Drain Looks Like
When thinking of a surgical drain, it's easiest to picture a tube that on one end is attached to a bulb and on the other end, is extending inside your body into the surgical area. The drainage tube will be held in place with a suture so that it doesn't accidentally slip out.
Within your body, the tube collects blood and clear lymphatic fluid that then moves into the bulb, where it can be measured, recorded, and then removed.
Fluid Within the Surgical Drain
You will use the drain to remove and measure the fluid multiple times a day and keep a record of how much blood and lymph is removed. Early on, the drainage is usually bright red, becoming thinner and changing to a straw-like color after the first few days.
As the volume of fluid decreases, swelling around your surgery site should decrease. When the fluid volume is 30 ml or less in a 24-hour period, you can have the drains removed. That said, even if you continue to have drainage greater than this, some surgeons still recommend removing the drains at around three weeks.
Mastectomy With Breast Reconstruction
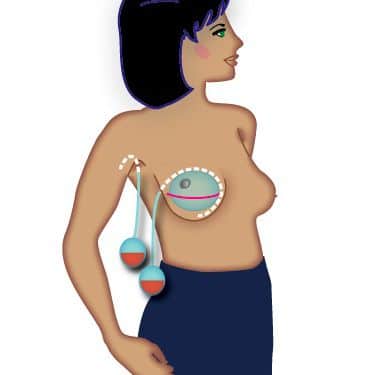
This illustration shows the location of two surgical drains. This is because the woman had a mastectomy with immediate breast reconstruction, using a tissue expander.
With that, one surgical drain has been placed around the temporary breast implant to collect blood and lymph.
In addition, the woman in the illustration has a sentinel node biopsy to check whether the breast cancer has spread to the lymph nodes, so there is a drain line close to her armpit. Depending on the results of your sentinel node biopsy your surgeon may also do a lymph node dissection removing further nodes.
Mastectomy Without Breast Reconstruction
For people who have a simple mastectomy without immediate reconstruction, there may be only one long incision that includes your lymph node biopsy as well as your mastectomy. Your surgeon may place surgical drains in your incision to help speed up your healing. Some people will have one drain and some will have more. If you have a bilateral mastectomy with lymph node biopsy you may have as many as five or six drains.
The bottom line is that while your surgeon may place a drain in a location somewhat different than those in the illustration here, the concept is the same—a surgical drain allowing excess fluid to be removed. This way you can heal well and rapidly and continue on your road to recovering from breast cancer.
By the American Cancer Society (Cancer.org)
Cancer cells tend to grow fast, and chemo drugs kill fast-growing cells. But because these drugs travel throughout the body, they can affect normal, healthy cells that are fast-growing, too. Damage to healthy cells causes side effects. Side effects are not always as bad as you might expect, but many people worry about this part of cancer treatment.
The normal cells most likely to be damaged by chemo are :
- Blood-forming cells in the bone marrow
- Hair follicles
- Cells in the mouth, digestive tract, and reproductive system
Some chemo drugs can damage cells in the heart, kidneys, bladder, lungs, and nervous system. Sometimes, you can take medicines with the chemo to help protect your body’s normal cells. There are also treatments to help relieve side effects.
Doctors try to give chemo at levels high enough to treat cancer, while keeping side effects at a minimum. They also try to avoid using multiple drugs that have similar side effects.
What do I need to know about side effects?
- Every person doesn’t get every side effect, and some people get few, if any.
- The severity of side effects (how bad they are) varies greatly from person to person. Be sure to talk to your cancer care team about which side effects are most common with your chemo, how long they might last, how bad they might be, and when you should call the doctor’s office about them.
- Your doctor may give you medicines to help prevent certain side effects before they happen.
- Some chemo drugs cause long-term side effects, like heart or nerve damage or fertility problems. Still, many people have no long-term problems from chemo. Ask your doctor if the chemo drugs you’re getting have long-term effects.
While side effects can be unpleasant, they must be weighed against the need to kill the cancer cells.
Be sure to talk to your cancer care team about which side effects are most common with your chemo, how long they might last, how bad they might be, and when you should call the doctor’s office about them.
What are common side effects?
Most people worry about whether they’ll have side effects from chemo, and, if so, what they’ll be like. Here are some of the more common side effects caused by chemotherapy:
- Fatigue
- Hair loss
- Easy bruising and bleeding
- Infection
- Anemia (low red blood cell counts)
- Nausea and vomiting
- Appetite changes
- Constipation
- Diarrhea
- Mouth, tongue, and throat problems such as sores and pain with swallowing
- Nerve and muscle problems such as numbness, tingling, and pain
- Skin and nail changes such as dry skin and color change
- Urine and bladder changes and kidney problems
- Weight changes
- Chemo brain, which can affect concentration and focus
- Mood changes
- Changes in libido and sexual function
- Fertility problems
American Society of Clinical Oncology (Cancer.Net)
Radiation therapy treats many types of cancer effectively. But like other treatments, it often causes side effects. These are different for each person. They depend on the type of cancer, its location, the radiation therapy dose, and your general health.
Why does radiation therapy cause side effects?
High doses of radiation therapy are used to destroy cancer cells. Side effects occur because radiation therapy can also damage healthy cells and tissues near the treatment area. Today, major advances in radiation technology have made it more precise, leading to fewer side effects.
For some people, radiation therapy causes few or no side effects. For others, the side effects are more severe. Reactions often start during the second or third week of treatment. They may last for several weeks after the final treatment.
Common general side effects
Radiation therapy is a local treatment. Therefore, it only affects the area of the body where the tumor is located. For example, people do not usually lose their hair from having radiation therapy. But if radiation therapy is aimed at a part of the body that grows hair, such as the scalp, a person may have hair loss.
Skin problems. Some people who receive radiation therapy experience dryness, itching, blistering, or peeling. But these side effects often depend on which part of the body received radiation therapy. If you develop skin problem, they usually go away a few weeks after treatment has finished. If skin damage becomes a serious problem, the doctor may change your treatment plan.
Fatigue. Fatigue is feeling tired or exhausted almost all the time. Your level of fatigue depends on whether you are having other treatments, such as chemotherapy. Learn more about how to cope with fatigue.
Long-term side effects. Most side effects go away after treatment. But some continue, come back, or develop later. These late effects may include developing a second cancer. However, the risk of having a second cancer because of radiation therapy is low. This risk is often smaller than the benefit of treating the primary, existing cancer.
Side effects specific to where radiation therapy is given
In addition to general side effects, some side effects of therapy depend on the type and location of the radiation.
Head and neck. If radiation therapy is aimed at a person’s head and/or neck, they may experience these side effects:
- Dry mouth
- Mouth and gum sores
- Difficulty swallowing
- Stiffness in the jaw
- Nausea
- A type of swelling called lymphedema
- Tooth decay. Learn more about dental health during cancer treatment.
Chest. Radiation therapy aimed at the chest may cause these side effects:
- Difficulty swallowing
- Shortness of breath
- Breast or nipple soreness
- Shoulder stiffness
- Cough, fever, and fullness of the chest. This is known as radiation pneumonitis and happens between 2 weeks and 6 months after radiation therapy
- Radiation fibrosis, which is permanent scarring of the lungs from untreated radiation pneumonitis. The radiation oncologist knows how to lower the risk of fibrosis in the planning process.
Stomach and abdomen. Radiation therapy aimed at the stomach or abdomen may cause these side effects:
- Nausea and vomiting
- Diarrhea
These symptoms will likely disappear after treatment. Your doctor can prescribe drugs for these side effects, and making changes to your diet may also reduce your discomfort.
Pelvis. Radiation therapy aimed at the pelvis may cause these side effects:
- Diarrhea
- Rectal bleeding
- Incontinence
- Bladder irritation
In addition, radiation therapy to the pelvis can cause different symptoms for men and women.
For men:
- Sexual problems, such as erectile dysfunction, which is the inability to get or maintain an erection
- Lowered sperm counts and reduced sperm activity from radiation therapy to the testes or prostate. This may affect the ability to father a child. Learn about ways to preserve your fertility.
For women:
- Changes in menstruation, such as stopping menstruating
- Symptoms of menopause, such as vaginal itching, burning, and dryness
- Infertility, which is the inability to conceive a child or maintain a pregnancy, if both ovaries receive radiation. Learn aboutways to preserve your fertility.
Radiation recall
Radiation recall is a rash that looks like a severe sunburn. Although rare, it occurs when certain types of chemotherapy are given during or soon after external beam radiation therapy.
The rash appears on the part of the body that received radiation. Symptoms may include redness, tenderness, swelling, wet sores, and peeling skin.
Typically, these side effects start within days or weeks of radiation therapy. But it can also appear months or years later. Doctors treat radiation recall with medications called corticosteroids. Rarely, you may wait until the skin heals before continuing chemotherapy.
Coping with side effects
Everyone’s experience with cancer treatment is different. Talk with your doctor or nurse about side effects that you may or may not develop before treatment begins. It is also important to continue talking with your health care team throughout your treatment schedule. There are many options for managing side effects. Your health care providers need to know you are experiencing them in order to help you feel better.
Cynthia DeMarco
MD Anderson Cancer Center (mdanderson.org)
Many cancer patients will receive chemotherapy infusions as a part of their cancer treatment.
Sometimes, chemotherapy is delivered safely through a standard (or “peripheral”) IV line. Other times, infusions must be administered through a central line catheter, such as a PICC, CVC or port.
How do these options differ? And which one is right for you? We spoke with Tam Huynh, M.D., chief of Vascular Surgery at MD Anderson, to learn more.
What are the differences between an IV, a port and a central line?
- A peripheral IV line (PIV, or just “IV”) is a short catheter that’s typically placed in the forearm. It starts and ends in the arm itself.
- A PICC line is a longer catheter that’s also placed in the upper arm. Its tip ends in the largest vein of the body, which is why it’s considered a central line. PICC stands for "peripherally inserted central-line catheter.”
- A CVC is identical to a PICC line, except it’s placed in the chest or neck. CVC stands for “central venous catheter.”
- A port is a catheter that’s implanted surgically under the skin on the chest. It’s another type of central line.
Which one should I get?
It depends on the type of chemotherapy you need and the time required to administer it.
- A PIV can be left in place for up to four days and can only be used with certain types of chemotherapy (those that don’t cause irritation or blistering, which can damage veins).
- A PICC line can be left in place for weeks or months, but must be kept dry at all times (even when showering). It also requires regular cleaning and maintenance to function well.
- A CVC can remain in place for weeks, months, or until treatment is complete. It must also be kept dry and regularly maintained.
- A port can stay in place for years. It requires only limited maintenance, which is performed by MD Anderson staff. And patients can shower — or even swim — with a port.
All central lines (PICC, CVC and port) can be used to deliver any type of chemotherapy.
Which patients should consider getting a port or a central line?
If you’ve had difficulty getting regular IVs placed, you may want to consider having a port or other central line installed. Most patients have had experience with PIVs and can report if it’s difficult to insert them. And as treatment progresses, it may become more and more difficult to place a PIV. So, it’s important to talk to your doctor about it before starting treatment.
You should also consider getting a port or other central line if you’ve had reactions to chemotherapy that was infused through a PIV — such as pain, redness or swelling at the IV site and/or streaking (redness/discoloration tracing along the vein).
Under what special circumstances might a doctor recommend a port or central line?
If you need a continuous infusion of chemotherapy through a portable pump at home, you’ll need a central line. These types of infusions cannot be given through a PIV, due to the high risks of chemotherapy leaking into surrounding tissues and accidental dislodging.
Your doctors may also recommend one based on the state or accessibility of your veins. If you already have small, weak or hard-to-find veins, or MD Anderson staff routinely have difficulty placing PIVs or drawing blood for lab work, a central line or port may be placed prior to starting treatment.
What’s the most common objection patients have to getting a central line? What do you tell them?
Most patients have concerns about care and maintenance. PICC lines and CVCs need dressing changes every week, and flushing is recommended daily.
At MD Anderson, we have resources to help patients and caregivers learn how to do this. We offer classes on how to care for central lines. Patients also can visit one of two walk-in Infusion Therapy Clinics (Main Building, Floor 8, Elevator C and Mays Clinic, Floor 8, Elevator U) for routine care and maintenance. And finally, home health care may be an option. Check with your MD Anderson case manager to see if your insurance policy covers it.
Since port placements require sedation and/or anesthesia in an operating room, some patients have concerns about having surgery. But other central lines can be placed in the clinic using local anesthesia. So, if you want to avoid general anesthesia, we typically recommend a PICC line.
How long do patients typically have to use a port or a central line?
Most patients keep their PICC, CVC or port until they’re done with treatment, but it’s different for every person. Ports are often requested because they allow patients more normalcy in their daily living and require less maintenance. But ports are not always the best choice. If you need a central line only for a few days to a few weeks, a PICC line may be recommended, since it’s the easiest to place and remove.
How long does it take for a patient to get a central line?
PICC lines and CVCs can usually be placed at MD Anderson’s Infusion Therapy Clinic within 24 to 48 hours of receiving an order from the physician. An implanted port takes up to a week to be placed, as it’s considered a surgical procedure. Those are only scheduled after you have a consultation with an oncologist.
What do patients report as the hardest aspect of having a port or central line? What advice do you give them?
For PICCs and CVCs, care can sometimes be a challenge. You have to keep the dressing clean, dry and intact at all times, so you have to cover it with plastic wrap and tape during showers, and you can’t take baths or go swimming.
Patients also complain about limitations to their activities. Exercising can be hard, because external catheters sometimes catch on things.
We remind patients that there are still some activities they can do, such as walking or cycling. We also note that ports allow patients more freedom, so talk to your oncologist if you’re interested in one to see if you’d be a good candidate.
How should patients care for their ports and central lines?
CVCs and PICCs require weekly dressing changes and daily flushing for maintenance. Ports are flushed after each use and only require flushing once a month when they are not being used regularly. No dressing changes are required with a port.
What myths or misconceptions about ports and central lines do you hear a lot?
Actually, there are two:
- Patients sometimes mention that they don’t want a port or central line because the infection rate or risk is high. While it’s true that there’s a risk of infection with any catheter, that risk can be decreased with proper care and maintenance. Mindful observation of the site will help catch any complications early on and produce better outcomes.
- Ports and central lines do not end with the tip of the catheter inside the heart. The tip of the catheter is located either in the superior vena cava (SVC) or at the atriocaval junction (ACJ), which is where that large central vein meetsthe heart.
What’s the one thing you wish patients knew about ports and central lines?
Ports and central lines are there to help you, and they are very safe ways of delivering chemotherapy.
The fabric, hidden pockets, snap enclosures, and designs of Eileen & Eva® pieces offer comfort and style right after surgery, during treatment and beyond. The buttery soft, breathable, anti-microbial fabrics handle hot flashes and night sweats beautifully, especially for sensitive skin. The hidden pockets hold post-surgery drains well, in both the Heal with Style Wrap, Chic Lounge Tunic and Laid-Back Lounge Shirt. For women undergoing chemo, the Heal with Style Wrap’s snap enclosures offer easy access to the PICC lines and ports that are used to administer medication. The slimming lines and ample draping allow for weight gain or lymphedema.
Every piece is designed to help her heal with style.
The fabric, hidden pockets, snap enclosures, and designs of Eileen & Eva® pieces offer comfort and style right after surgery, during treatment and beyond. The buttery soft, breathable, anti-microbial fabrics handle hot flashes and night sweats beautifully, especially for sensitive skin. The hidden pockets hold post-surgery drains well, in both the Heal with Style Wrap, Chic Lounge Tunic and Laid-Back Lounge Shirt. For women undergoing chemo, the Heal with Style Wrap’s snap enclosures offer easy access to the PICC lines and ports that are used to administer medication. The slimming lines and ample draping allow for weight gain or lymphedema.
Every piece is designed to help her heal with style.
You need soft clothing that offers coverage, holds drains (until they are removed), and accommodates hot flashes, lymphedema and weight gain. You deserve pieces that are simple and elegant, that are interchangeable and that allow for your individual styling preferences. Because you will be recovering over many weeks or months (depending on your treatment protocol), your wardrobe will need to maintain its structure through multiple washings and the wear and tear that happens over time.
You want breathable, soft, moisture-wicking and antimicrobial fabric. There is no substitute for Eileen &Eva’s proprietary Tencel blend. We thoroughly researched the best options for our customers and we wound up creating our own version due to our extensive demands of Eileen & Eva® garments. You can read more about it in this blog.